Global Ageing Statistics: Falls and Injury for Seniors and Elderly

Data on falls in the elderly
Falling is the action of involuntarily collapsing to the ground. Falls have been associated with sensory, neuromuscular and bone and joint deficiencies (Dargent-Molina and Bréart, 1995) and falls resulting in trauma are a major cause of mortality and morbidity. In the elderly, falls are the main cause of accidental death (Dargent-Molina and Bréart, 1995; CFES, 1999). In industrialized countries, it is estimated that a third of elderly persons aged 65 or more and living at home fall each year (DargentMolina and Bréart, 1995) and this proportion increases with age. Women are approximately two times more likely to fall than men, although this difference between men and women disappears as age increases; after 80 years, proportions become identical, and after 85 years, relative frequencies are comparable (Dargent-Molina and Bréart, 1995). Although physical consequences of falls are extremely variable, they frequently provoke a loss of self-confidence that may in turn accelerate the loss of functional capacity (Vignat, 2001). For some individuals, a fall will result in decreased mobility and increased dependence. Fractures occur in 5% of falls, the most serious of which are proximal fractures of the femur (less than 1% of cases) Other injuries necessitating medical attention, including dislocations, sprains, hematomas and deep wounds requiring stitching, will occur in 5% to 10% of falls.
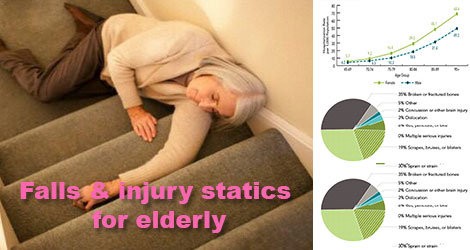
In the most serious cases, falls may result in a significant loss of functional capacity that may in turn necessitate post-hospitalization placement in institutionalized care. Fall frequency and consequences can be visualized in the form of a pyramid. This schema was developed using data from studies done in Quebec and furthermore integrates the results of epidemiological studies (Dargent-Molina and Bréart, 1995). It illustrates the impact of falls on the elderly population. In 1998 in Quebec, more than 300,000 falls were reported in a population of more than a million people aged 65 or older. More than half of these falls were recurrent. In all, 50,640 falls resulted in injury that necessitated medical consultation, 12,681 led to hospitalization and 600 resulted in death. France’s elderly population counts 9 million individuals and falls are estimated at 2,700,000. These result in 450,000 injuries, 110,000 hospitalizations and more than 5,000 deaths. Similar data were not available from Belgium and Switzerland, but these proportions from Quebec and France most likely correctly illustrate the significance of falls in the elderly.
Falls are a result of a wide range of complex and interdependent factors. Since the 1980s, over 400 fall risk factors have been described by researchers. The relative importance of the various risk factors and their interactions are not currently well described. Studies do suggest however that the importance of any one factor is relatively small and that falls are more so a result of several factors acting together Thus, the risk of falling within the year increases linearly with the number of risk factors: from 8% when no risk factors are present to 78% when four or more risk factors are present. In the scientific literature, risk factors are often presented in terms of three interactive dimensions, i.e. state of health of the elderly person, behavior, and environment. To ease the use of this Guide, these three dimensions are presented separately. However, cross-references will be provided whenever possible to illustrate the multifactorial nature of falls and the numerous interactions between risk-factors. Although the roles of a certain number of risk factors in falling are better understood today, information is still lacking for others. For example, research into behavioral (e.g., risk-taking, nutrition) and environmental factors is immature, as these studies are often difficult to design and their results difficult to measure.
The frequency of falls increases with age. It is estimated that each year, a third of the elderly over 65 and half of those over 85 will fall once or more. The combined effects of aging and age-related diseases augment the risk of falling and the gravity of resulting injury (Dargent-Molina and Bréart, 1995). Over a certain age, even those who do not present any particular risk factors should engage in a certain number of preventive initiatives, in particular regular physical activity. Other sociodemographic factors that increase the risk of falls have been variably demonstrated in studies. Although some of these factors cannot be modified, or cannot be easily modified, they do provide information for determining the elderly populations that should receive access to fall prevention programs. Women are at a greater risk of falling than men, which may be explained by a more pronounced physical fragility. People living alone, often elderly women, may run an additional risk after a fall with an associated increased risk of serious consequences, that of spending additional time on the ground, which increases the risk of loss of autonomy. This is more pronounced in elderly individuals who live alone or who do not receive social support.








